In July 2016, the Office for Health Economics and the European Personalised Medicine Association published a white paper titled: “The Value of Knowing and Knowing the Value: Improving the Health Technology Assessment of Complementary Diagnostics”. This publication did not receive a great deal of attention at the time, but it raises some interesting points related to genomic testing that are worthy of consideration by a wider audience. In particular, it highlights several things that we currently do reasonably well in health economics and genomics, as well as some areas in which we need to improve evidence generation, suggesting a future research agenda in this field.
The main aim of the report was to develop more comprehensive framework for assessing the potential value contribution of complementary diagnostics, with a key focus on the value of knowing. This builds on earlier work on value frameworks, previously considered in this blog. For the purposes of this report, companion diagnostics were defined quite broadly, including both tests that enabled risk stratified screening and also tests that reduced uncertainty.
A key point raised early in the paper is that it is difficult to reconcile a study of the value of knowing with the narrow value framework commonly applied by HTA bodies when evaluating both medicines and diagnostics. There is a compelling argument that the same framework should be applied in both cases if the costs associated with new interventions in either category will be met by the same overall budget. Therefore, if a wider value framework is judged to be appropriate for complementary diagnostics, this should also be applied for medicines (with appropriate budgetary adjustments). Resolving this issue is probably beyond the scope of the white paper. That said, there is an interesting section towards the end of the report which describes the differences between the UK and French systems in this regard, and this is worth a read.
Moving on, section two of the white paper contains the material of most interest to this blog. The authors describe ten elements of value for complementary diagnostics, as per the following figure.
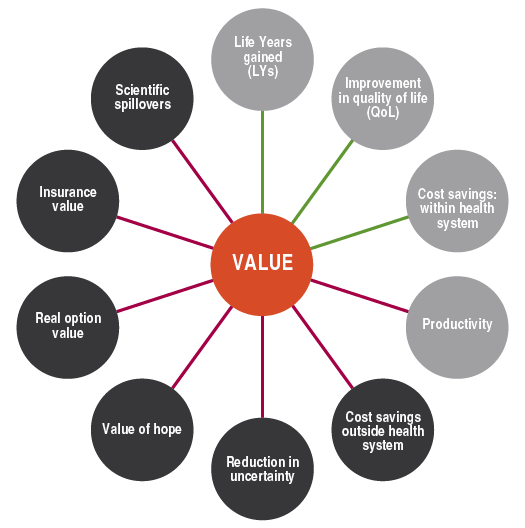
Of these elements, health gains, quality of life gains, costs and productivity have been addressed in slightly more detail in genomics already, so I’m going to mostly ignore them. However, the report makes a couple of points in relation to health gains that are worth noting in a genomic context.
First, the authors note that health gains are more likely when the outcome associated with a diagnostic is binary (e.g. patient is definitely a responder or non-responder). This is unlikely to be the case in many genomic testing scenarios, particularly those in which a range of SNPs are evaluated to generate a polygenic risk score.
Second, the authors comment that “the health gain resulting from adding a diagnostic to the care pathway depends on the interaction between the test results and the complex choices and care pathways that are downstream”. This is a key issue for genomic diagnostics. In part, this is because care pathways both before and after the introduction of a genomic diagnostic can be particularly complex. The key issue, however, is that the preferences of patients can influence uptake, and, as the authors note: “if patients are more certain that they are likely to benefit, then a greater share of the population may use a technology”. The lack of evidence (both economic and non-economic) currently available to support the widespread use of genomic testing creates a great deal of uncertainty in this field, which means that it is crucial that economic evaluations of genomic tests account for this factor.
Beyond health gains, there are three elements of value that are of particular importance in genomics. I don’t think we do a particularly good job of capturing any of these elements in our analyses.
Value from reduced uncertainty
First, diagnostics reduce uncertainty, which generates value. Reduced uncertainty allows R&D investment to be optimised and healthcare resources to be more efficiently allocated according to need. It also benefits risk-averse individuals, facilitates better planning, and changes the behaviour of clinicians and patients. This source of value is particularly important in genomic testing, indeed, sometimes this is the only source of value from conducting a genomic test (e.g. testing patients with unexplained learning disabilities). It is crucial that health economists do a better job of quantifying this value going forward.
Real option value
Option value captures the idea that by undergoing one healthcare intervention (e.g. a test or a treatment), a patient increases their chances of benefitting from a better test or treatment in the future. This benefit could arise because new technologies become available in the future, as is often the case in genomics. It could also arise because new information is discovered that enables existing genomic test results to be reinterpreted, creating clinical utility (e.g. by changing treatment). This is not a factor that is currently widely considered in genomic economic evaluations.
Scientific spillovers
Finally, scientific spillovers are defined by the authors as information externalities that result in new adaptations. For example, DNA samples collected via a genomic test can be of value to researchers and clinicians working in different contexts, facilitating the discovery of new treatments and improved tests. The scope of HTAs of genomic tests does not currently extend to capturing these benefits.
Ok, wrapping this up. The authors move on to describe the relevance of these elements to some case studies, which mainly serves to highlight how infrequently these elements of value are considered, even when they are potentially important. They end with two key policy recommendations:
- Value frameworks used to assess complementary diagnostics require a more comprehensive perspective in order to integrate less tangible benefits. In many cases, this requires the analyst to augment traditional HTA tools with other approaches (e.g. contingent valuation) to capture the value of these other elements.
- HTA agencies should assess the use of ‘coverage with evidence development’ agreements and reflect on “the current tendency in the US toward pragmatic and flexible approaches for the assessment of medical devices”. This could take the form of allowing the use of data generated in e.g. adaptive trials, which are particularly appropriate for genomic tests.
I’m not convinced that this report is sufficient, by itself, to lead to changes in how HTA is conducted for genomic tests. However, it does form part of a growing body of evidence arguing for change, and the ideas contained within the white paper will underpin many a discussion on this topic in the next five years.

Information is very useful. Need value to evolve..
Hopefully this website will always give benefit to society and advancing the community in the future.
Regards,
Utuh Wibowo
http://www.utuhwibowo.com
LikeLike